Diabetes is a disease in which the body does not produce any or enough insulin, or is not able to use insulin effectively. Insulin is a hormone which combines with glucose (sugar) in the blood. It helps glucose or sugar to enter the body’s cells to be used for energy.
Type 1 accounts for only 5-10% of people with diabetes. People with type 1 diabetes do not produce insulin. This type of diabetes usually begins in childhood or before age 30. A person with type 1 will need to take insulin daily in addition to eating well and being active.
Type 2 diabetes is the most common type and accounts for 90-95% of people with diabetes. In type 2 diabetes, the body does not make enough insulin or is not able to use it. This type of diabetes is most often found in people over age 45, but is becoming more common in younger people, including children.
In the early stages, people with type 2 can often maintain a normal blood glucose by healthful eating and regular activity. However, as the disease progresses, oral pills or insulin are usually needed to achieve target blood glucose goals.
Gestational diabetes is a special type of diabetes that occurs in a small number of pregnant women. After pregnancy, blood glucose levels usually return to normal. However, a woman who has had gestational diabetes, has a greater chance of developing type 2 diabetes later in life, especially if she is overweight and sedentary.
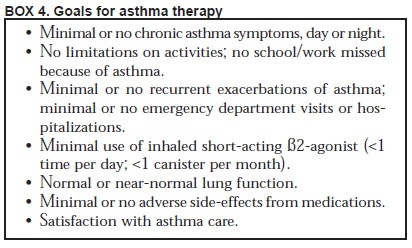
Taking care of your diabetes will help you feel better and may help reduce or delay the problems associated with diabetes such as heart attack, stroke, blindness, kidney disease or losing a foot or leg. The management of diabetes focuses on controlling the diabetes ABCs:
• A1C (Pronounced A-one-C): A laboratory blood test that measures your average blood glucose level over
the past three months.
• Blood Pressure: High blood pressure makes your heart work too hard.
• Cholesterol: LDL or bad cholesterol builds up and clogs your arteries and HDL or good cholesterol helps remove cholesterol from your blood vessels.
You and your health care team will need to monitor your ABCs. The chart below lists recommended target numbers.
Working with your health care team, you can manage your diabetes to achieve your target goals. One of your team members is the pharmacist.
Our pharmacist can answer questions about diabetes products, including blood glucose meters, medications and foot care products. Another member of your health care team is a Registered Dietitian (RD), especially one with Diabetes Education Certification (CDE). Working with a dietitian, you can learn how to balance your food, activity and medication. Together you and your dietitian can develop an individualized meal plan based on your food likes and dislikes as well as your lifestyle that will help you achieve your target ABCs.
But remember, you are the leader of your diabetes care team.
Controlling diabetes is a balance of healthful eating, regular activity and medication. Checking your blood sugar lets you know if you need to adjust any of the components.
To help control your diabetes you may need to check your own blood glucose at home with a meter. It tells you what your blood glucose is at the time you do the test. Checking at different times of the day – before
and after meals, before and after exercise, before bed - allows you to look for patterns. Most meters today read the blood sample results as plasma rather than whole blood glucose values. Make sure you know whether your meter provides plasma or whole blood results.
diabetes overview
Diabetes meal planning
Eating right with diabetes is no longer about following a “diet”. It is about making healthy food choices, and the foods that are good for you are also good for everyone in your family.
• The basic principles of diabetic meal planning are:
1. Do not skip meals. Skipping meals can cause your blood glucose to drop if taking certain diabetes medications. And people who skip meals tend to overeat at the next meal which can raise your blood glucose.
2. Control carbohydrate intake. Carbohydrates in foods are what most affect blood glucose levels. That does not mean you should not eat carbohydrates, but rather, control how much is eaten at meals and snacks.
Carbohydrates come from many foods:
• Starches, such as bread, rice, cereals, pasta, starchy vegetables (such as potatoes, corn and green peas), dried beans and peas.
• Natural sugars found in milk (lactose) and fruit (fructose).
• Added sugars such as table sugar, corn syrup, molasses, dextrose, honey, high fructose corn syrup, and fruit juice concentrate.
3. Eat a variety of foods. Consume the recommended number of servings from each of the food groups to ensure you get all the nutrients you need on a daily basis. See the Diabetes Food Pyramid on page 10.
4. Eat less saturated fat, trans fat and cholesterol. Saturated fat, trans fat and to a lesser extent, cholesterol in your diet may increase your blood cholesterol level, which in turn may increase your risk of heart disease.
Because there is a strong connection between diabetes and heart disease, it is important to maintain a normal blood cholesterol level.
• Saturated fats are usually solid at room temperature and found mainly in animal foods such as meat fat, poultry skin, lard, butter, cheese, and whole and 2% milk.
• Trans fats are produced when oils (unsaturated fats) are made harder through a process called hydrogenation. Trans fats are found mainly in commercial baked goods, fried foods, and stick margarines.
• Dietary cholesterol is found only in animal foods, and the most concentrated sources are egg yolks, organ meats, shrimp and squid.
5. Eat more fiber. People with diabetes need to eat more fiber just like everyone else. Many people routinely eat only about half the recommended amount of fiber per day. A diet rich in fiber fills you up and helps lower blood cholesterol levels. Fiber comes from many foods:
• Grains and grain products especially whole grain breads and cereals.
• Fruits and vegetables. Fiber is found in all fruits and vegetables including fresh, frozen, canned, and dried. Cooking does not lower the fiber content of the food, but juice has little or no fiber.
• Cooked dried peas and beans such as lima, kidney, black, pinto, and navy beans, and split peas and chick peas are very high in fiber – about 5 grams or more per 1/2 cup serving.
Slowly increase the amount of fiber you eat. Aim for 21-38 gramsper day or 14 grams per 1000 calories consumed. Be sure to consume water and other beverages throughout the day as you increase your fiber
intake. Thirst is the best indicator to drink more fluid.
6. Maintain a healthy body weight. If overweight, aim for a moderate weight loss of 5 to 10% of your current weight. This amount of weight loss can help improve your blood glucose, blood cholesterol and blood pressure.
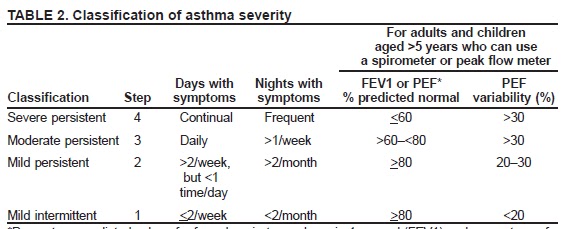
The government classifies weight by Body Mass Index (BMI). A healthy BMI is 18.5 – 24.9. To lose weight, eat less and move more.
BMI Classification
<18.5 Underweight
18.5 - 24.9 Normal
25.0 - 29.9 Overweight
30.0 - 39.9 Obesity
>40.0 Extreme obesity
This formula can be used to calculate your BMI
How do I set up a meal plan?
A meal plan is a guide that tells you how much and what kinds of food to eat at meals and snacks. A good meal plan should fit in with your eating habits and schedule. You and your dietitian should work together to design a meal plan that’s right for you and includes foods you enjoy.
Understanding your meal plan allows for flexibility so you can eat out, use convenience foods and allow for special events. It will also help you adjust for changes in your schedule, such as days when meals may
be delayed or when you are feeling ill.
diabetes overview
Carbohydrate counting
Carbohydrate counting is a meal planning tool that allows you to eat carbohydrates in amounts that keep your blood glucose in your target range.
A dietitian can help you determine the total amount of daily carbohydrate that is best for your sex, age, and activity level and how to distribute it through the day.
The first step: Know which foods contain carbohydrates. Carbohydrates include both starches and sugars. It is best if most of the carbohydrates you eat come from healthy foods like bread, cereals, grains, cooked dried beans and peas, starchy vegetables, fruits, milk, and yogurt. These foods contain vitamins, minerals and fiber. Sugars and sweets have little nutritional value and are often high in fat. It’s OK to eat sweets once in a while, but when you do eat sweets you must eat less of other carbohydrates, rather than just add the sweets to your meal plan.
The second step: Learn serving sizes. A serving of starch, fruit or milk is the amount of food that provides about 15 grams of carbohydrate and is referred to as 1 carbohydrate choice or serving. See the Diabetes Food Pyramid on p.10 to learn serving sizes for foods in the starch, fruit and milk groups. It will help to measure or weigh foods until you can judge them by looking at a portion on your plate.
The third step: Spread carbohydrate throughout the day. Based on the total amount of carbohydrate in your meal plan, divide your daily carbohydrate up into meals and snacks. To avoid fluctuations in your blood glucose, it is best to eat about the same amount of carbohydrate at each meal and snack and to eat meals and
snacks at about the same time each day.
How many carbohydrates choices do you need? A general guide is:
Women: 45-60 grams (3-4 choices) per meal; 0-30 grams (0-2 choices) per snack
Men: 60-75 grams (4-5 choices) per meal; 0-30 grams (0-2 choices) per snack
Checking your blood glucose levels before and after different meals will help you learn the amount of carbohydrate in meals and snacks that works for you. If you need to lose weight or are very active, you may need fewer or more servings than recommended above.
The Diabetes Food Pyramid
Another approach to meal planning is to use the Diabetes Food Pyramid (above) as a guide of what and how much to eat. This allows for a variety of foods every day and can be used by the whole family.
The Diabetes Food Pyramid groups foods by carbohydrate content so it works better for people with diabetes. It is different from the USDA My Pyramid you may have seen in government publications, pamphlets or on food packaging.
How many servings?
The number of servings needed from each food group in the Pyramid is given in ranges, rather than a single number. For example, the bottom group Grains/Beans/Starchy Vegetables suggests 6 or more servings per day. Why? Because we are very different people. Smaller people and older people need less food than larger people, younger people or very active people. Thus, a small, older woman will need fewer servings per day than a younger, large man.
Individuals may need to make adjustments according to their own needs and blood sugars. Your health care team, particularly your dietitian, may prescribe a slightly different plan for you based on your target goals.
The plate method Another meal planning method is the plate method. With this method, no measuring is required. Instead, your plate determines the correct portion. Divide a plate into quarters. For lunch or dinner, use one quarter of the plate for Meat and Meat Substitutes, one quarter for Grains, Beans & Starchy Vegetables and the remaining half for Vegetables. For breakfast, use one quarter of the plate for Meat & Meat Substitutes if desired, and one half for Grains, Beans & Starchy Vegetables. A glass of milk, or a serving of fruit may be added to any of the meals or reserved for snacks.
Too many people cover their plate with large servings of starch or protein foods and skimp on vegetables. This way of eating can lead to too many calories, too much carbohydrate and too much saturated fat.
How sweet it is
Sugar substitutes or sugar replacers include nonnutritive sweeteners and sugar alcohols. They can both replace sugar sweeteners in foods and drinks.
• Nonnutritive sweeteners – No calories or carbohydrates There are five nonnutritive sweeteners approved by the Food and Drug Administration (FDA) for use in foods and beverages:
• Acesulfame potassium (K)
• Aspartame
• Neotame
• Saccharin
• Sucralose
These nonnutritive sweeteners are calorie-free (except for aspartame which is very low in calories). Products that use these sugar substitutes include diet soft drinks, sugar-free gelatins, powdered drink mixes, chewing
gum, jellies, jams, pancake syrup and light yogurts. They are also available as tabletop sweeteners.
• Are nonnutritive sweeteners safe?
The five nonnutritive sweeteners currently on the market were extensively tested before they were approved by the FDA. They are considered safe for everyone, including children and pregnant women, in amounts that consumers would typically consume of them. However, people with phenylketonuria (PKU), a rare genetic disease, need to limit their intake of aspartame.
• Sugar alcohols (Polyols) – Contain calories and carbohydrates Sugar alcohols are carbohydrates that sweeten with fewer calories per gram than sugar. Also called polyols, sugar alcohols are neither sugars nor alcohols. Sugar alcohols include:
• Sorbitol, mannitol, xylitol, erythritol, D-tagatose
• Isomalt, lactitol, maltitol, trehalose
• Hydrogenated starch hydrolysates (HSH)
Sugar alcohols are often used in sugar-free or no-sugar-added foods such as gum, cookies, and ice cream.
Currently, there are two low-calorie sweeteners made from the sugar alcohol erythritol - ZSweet and Sun Crystals - available as tabletop sweeteners in some stores and on the internet.
• Stevia
Stevia is a calorie-free sweetener made from a plant in South America. FDA has not approved stevia for use as a nonnutritive sweetener in the United States for lack of scientific evidence to assure its safety.
However, stevia is sold as a dietary supplement, which does not require FDA approval. Check with your health professional before using it.
• How do nonnutritive sweeteners or sugar alcohols fit into your meal plan?
Nonnutritive sweeteners and sugar alcohols can help lower the amount of carbohydrate in foods and allow for more flexibility in your meal plan. However, sugar-free or no-sugar-added does not mean carbohydratefree or low-calorie. Sugar-free or no-sugar-added means that no sugar sweeteners such as white sugar, brown sugar, honey, syrup, molasses, high fructose corn syrup or fruit juice concentrate have been used in
the food or drink.
Often times, a sugar-free or no-sugar-added food has as many calories, and grams of fat and carbohydrate as the regular product. Check the Nutrition Facts label to determine how a sugar-free food or drink fits into your meal plan and/or carbohydrate budget. For example, sugar-free gum is calorie-free and carbohydrate-free, and can be consumed as a free food. In contrast, sugar-free cookies contain calories, fat and carbohydrate, and must be counted in your meal plan and/or carbohydrate budget, not eaten in addition to it.
Using the Nutrition Facts label
Serving Size: The serving size is the first thing you should look at. All the numbers in the Nutrition Facts box are based on this serving size.
If you eat more or less than this amount, you must adjust the numbers accordingly. Be aware that the serving size on the food label may not be the same as the serving size in your food plan.
% Daily Value (%DV): %DV is a useful tool for comparing foods.
If the %DV is 5% or less, it is low in that nutrient. If the %DV is
20% or more, it is high in that nutrient.
Total Fat: Look at the grams of total fat as well as the grams
of saturated fat and trans fat.
• A low fat food has 3 grams or less fat per serving.
• A low saturated fat food has 1 or less grams saturated fat per serving and no more than 15% calories from saturated fat.
• Trans fat: Try to eat as little as possible because it increases your risk of heart disease.
Sodium: Limit sodium to help reduce your risk of, or help control, high blood pressure. The recommended intake for healthy adults is 2300 mg sodium per day. For people with high blood pressure, the recommended
intake is 1500-2000 mg sodium per day.
Total Carbohydrate: Look at the grams of total carbohydrate.
It is the grams of total carbohydrate that needs to be counted intoyour meal plan, not the grams of sugar. Remember, 15 grams of carbohydrate is the same as one carbohydrate choice or serving.
The grams of sugar and fiber (and sugar alcohols if present) are indented under total carbohydrate because they are included in the total.
• If a food contains 5 or more grams of dietary fiber, you can
subtract half the fiber from the total carbohydrate grams
to get a more accurate carbohydrate count.
• If a food contains 5 or more grams of sugar alcohols,
you can subtract half the sugar alcohol content from
the total carbohydrate grams to get a more
accurate carbohydrate count.
• A free food is any food that contains less than 20 calories and less than 5 grams of carbohydrate per serving.
Shopping list
The first step to eating well is shopping right. You can find a wide selection of healthful foods at your supermarket.
At Stop & Shop, it is easy to find healthy foods. Just look for the Healthy Ideas symbol on the shelf tag! A Healthy Ideas food must meet strict criteria. A Healthy Ideas food will be low in total fat, saturated fat, and cholesterol and free of artificial trans fat. A Healthy Ideas food is also controlled in sodium and sugar and must provide at least 10% of the Daily Value for either protein, fiber, calcium, iron, vitamin A or vitamin C.
For complete criteria, visit our website, stopandshop.com or pick up a Healthy Ideas brochure at your store.
diabetes overview
Fruits and Vegetables
• All fresh, raw fruits and vegetables are healthy choices.
• Choose canned fruits in light syrup or juice.
• Choose no-salt-added canned vegetables or those with the Healthy Ideas symbol.
• Choose whole fruits over fruit juices.
• When buying juice, look for 100% juice (those with the Healthy Ideas symbol). Limit juice if overweight, because it has as many calories as regular soda.
• Choose plain frozen vegetables over those with sauce.
• Choose more dark green and deep yellow vegetables.
• To save time, buy pre-washed and pre-cut vegetables and fruits.
Meat, Poultry, Seafood and other Protein Sources
For the healthiest choices, look for the Healthy Ideas symbol. Only Extra Lean meats, with less than or equal to 5 grams total fat, 2 grams saturated fat, and 95 mg cholesterol per reference serving* qualify as a
Healthy Ideas food. Lean meats, with less than or equal to 10 grams total fat, 4 grams saturated fat and 95 mg cholesterol per reference serving* are good choices too.
• Choose cuts with the words “loin” or “round” in the name, e.g. top round or pork tenderloin.
• Choose 96% or 93% lean ground beef. Fresh ground turkey breast and 93% lean ground turkey are great choices also.
• Limit high fat meats such as ribs, corned beef, sausage or bacon.
• Buy skinless poultry parts or remove the skin before cooking.
• When buying fish and shellfish, look for fresh, plain frozen or canned in water instead of oil, for fewer calories. Skip the breaded or batter-dipped frozen fish.
• Include at least two seafood meals per week for heart health.
• Canned and dried beans (legumes) are high in fiber and good sources of protein.
• Peanut butter and other nut butters are another good alternative to animal protein. To qualify for the Healthy Ideas symbol, peanut and nut butters must be free of any added sugar.
• Choose egg substitutes for protein without fat and cholesterol.
• Look for soy products with at least 8.25 grams of protein per reference serving*.
Deli
• Look for deli meats with the Healthy Ideas symbol. These meats have less than 3 grams total fat and less than 1 gram saturated fat per serving.
• Look for lower sodium deli meats at the service deli.
• Choose roast beef, turkey, chicken and ham over bologna, salami, or pepperoni.
• Choose hot dogs with 3 grams of fat or less per serving (look for
the Healthy Ideas symbol). Chicken and turkey franks do not always have less fat than beef franks.
Breads, Cereals and Grains
• Choose breads that list whole grain or whole wheat flour as the first ingredient and contain at least 2.5 grams of fiber per serving.
• Look for whole grain cereals with at least 5 grams of fiber, and no more than 12 grams of sugar per serving.
• Choose quick oats or old fashioned oats over instant oatmeal varieties that have more sodium and sugar.
• Choose whole grain crackers. Go easy on cheese crackers, peanut butter crackers, and butter crackers.
• Choose whole grain pastas and whole grain blends.
• Choose brown rice and other whole grains such as bulgur and quinoa.
• Prepare rice and pasta mixes without added fat and salt.
Dairy
• Choose low fat and nonfat dairy products and plain or light yogurts.
• Nonfat milk meets the strict criteria of Healthy Ideas. Low fat milk (1%) has more saturated fat but is a good choice also.
• Limit 2% or whole milk and higher fat dairy products.
• Look for nonfat or light yogurt.
• Look for cheeses with no more than 3 g saturated fat.
• Look for light or diet margarine and cream cheese.
• Buy evaporated skim milk as a substitute for cream in coffee and recipes.
Convenience and Frozen Foods
• Frozen dinners with the Healthy Ideas symbol on the shelf tag are low in fat, saturated fat and cholesterol, and controlled in sodium (less than 600 mg per federal reference serving size*).
• Look for pasta sauces with the Healthy Ideas symbol. All Healthy Ideas pasta sauces are low fat, less than 480 mg sodium per refernce serving and are free from added sugars.
• Select broth or bean based soups over cream soups or Ramen-type soups.
Snacks and Sweets
Snacks and sweets are meant to be extras in your diet and eaten in moderation. Many snacks and sweets do not provide at least 10% of the Daily Value for a Healthy Ideas nutrient and therefore do not qualify for the
Healthy Ideas symbol. However, here are some tips to help you make good choices when you shop for these items.
• For low fat snacks, choose light microwave popcorn, pretzels and rice cakes.
• Look for low fat cookie choices including animal crackers, graham crackers, fig bars, ginger snaps, and vanilla wafers.
• Choose granola and cereal bars with at least 2.5 grams of fiber and no more than 1 gram of saturated fat and 0 grams of trans fat.
• Nuts are a healthy snack, but limit quantities.
• Choose nonfat puddings.
• Select low fat frozen desserts like light ice cream, frozen yogurt, sherbet, sorbet, Italian ice, popsicles, and fruit bars.
• No Sugar Added sweets such as sugar-free gelatin and popsicles can be a good choice, but always read the grams of total carbohydrate on No Sugar Added products.
Fats and Oils
• Choose soft margarines or spreads with 0 grams trans fat.
• Choose light or reduced fat salad dressings.
• Choose canola oil or olive oil for cooking.
• Choose light or reduced fat mayonnaise.
Be active each day
Physical activity is like medicine – but it costs nothing and has no negative side effects. Regular physical activity can help:
• Improve insulin sensitivity and lower blood sugars
• Achieve and maintain a healthy weight
• Improve blood pressure and blood cholesterol levels
• Relieve stress and improve emotional well-being To be physically fit, there are three things you need to work on:
aerobic endurance, muscle strengthening, and flexibility.
Aerobic endurance exercises increase breathing and heart rate, and help burn calories. Aerobic activities should be done most preferably all days of the week, for at least 30 minutes. Work hard enough to elevate
your breathing and heart rate, but not so hard you can’t carry on a conversation. Examples include brisk walking, jogging, bicycling, swimming, and rowing. An alternative to counting minutes is to get a step counter and count steps. For good health, aim for 10,000 steps daily, for weight loss aim for 12,000 – 15,000 steps daily.
Muscle strengthening exercises build muscle, maintain bones, and increase body metabolism, which helps with weight control. You can go to a gym and lift weights or use hand/ankle weights at home. Select a weight you can lift 8 times in good form before you have to stop and rest your muscles. Muscle strengthening exercises should be done 2 to 4 times per week in sets of 1 to 3 with 8 to 12 repetitions per set using arms, legs and trunk, e.g. arm lifts, leg curls and crunches/push-ups.
Flexibility (stretching) exercises help keep your body limber and reduce muscle stiffness. Stretching should be done slowly, without jerking.
Hold the stretched position for at least 10 seconds. Do 4 to 6 stretching exercises per session. Stretch after doing your endurance and muscle strengthening exercises.
diabetes overview