diabetes mellitus
Diabetes
A condition in which excessive amounts of some substances are excreted from the body. The term may refer to either of two unrelated diseases, diabetes mellitus and diabetes insipidus. The word diabetes derives from the Greek for siphon, a reference to the copious urine excretion that characterizes this affliction. In common usage, the term diabetes is synonymous with diabetes mellitus.



Diabetes Mellitus
Diabetes mellitus is a disease of abnormal carbohydrate metabolism in which glucose cannot enter the body's cells and be utilized, and therefore remains in the blood in high concentrations. Mellitus is the Latin word meaning honey, and is applicable because the urine of patients with diabetes mellitus has a sweet taste, distinguishing this disease from diabetes insipidus, in which large volumes of dilute, almost colorless and tasteless urine are passed. In diabetes mellitus the excess sugar in the blood (hyperglycemia) leads to the excretion of sugar in the urine (glycosuria), a cardinal diagnostic symptom. Glycosuria in turn causes the excretion of large amounts of urine (polyuria), which results in dehydration and intense thirst (polydipsia). Although blood glucose is high, it cannot enter the appetite-regulating cells of the hypothalamus; hunger is therefore great, and the diabetic person tends to eat constantly (polyphagia). But because glucose cannot enter and nourish the cells, body tissues are subjected to the equivalent of starvation; rapid weight loss occurs, part of which is due to the excretion of water in urine. See also: Carbohydrate metabolism
diabetes mellitus
Varieties
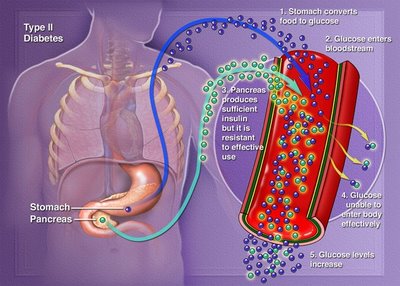
Diabetes mellitus appears in two varieties, each with its own cause: diabetes mellitus type I (formerly known as juvenile onset diabetes), caused by deficiency of the pancreatic hormone insulin (whose chief function is to promote the entry of glucose into cells); and diabetes mellitus type II (formerly known as maturity onset diabetes), in which insulin is available but cannot be properly utilized.
Diabetes mellitus type 1
diabetes mellitus type 1
Of the two forms of diabetes, type I is initially the more serious and less common, afflicting approximately 1 in every 600 children. The incidence varies among countries. The highest incidence is seen in Finland and Sweden, and some of the lowest in Korea and Mexico. The United States and Canada are included among the highest. Although it usually appears before the age of 20, type I diabetes can strike at any age. It is caused by a significant shortage or complete lack of insulin secretion. The endocrine cells normally responsible for insulin production are found in the pancreas, but have nothing to do with the ordinary digestive functions of that organ. They occur as islands of endocrine tissue, called islets of Langerhans, scattered throughout the substance of the pancreas. The islets consist of at least three cell types, each of which secretes a different hormone important in regulating carbohydrate metabolism. The alpha cells produce glucagon, which elevates blood glucose; the beta cells produce insulin; and the delta cells produce somatostatin, a hormone that appears to participate in controlling the activity of the alpha and beta cells.
In type I diabetes the beta cells are destroyed, possibly by the attack of the body's own immune system or by virus infection; victims of type I require daily insulin injections to survive. Insulin must be injected rather than taken orally because it is inactivated by the enzymes of the digestive system. Without insulin therapy, a patient with type I diabetes will inevitably deteriorate into a condition of ketosis (presence in the blood of ketone bodies, the metabolic intermediates of fat metabolism) and acidosis (dangerously acidic blood pH). Ketoacidosis, as the combined condition is called, leads rapidly to coma and death in the untreated diabetic.
When Frederick G. Banting and Charles H. Best succeeded in purifying insulin from animal pancreatic tissue in 1921, type I diabetics were given their first chance at living a normal life-span. Today type I diabetics are routinely treated by injections of insulin. Human insulin became increasingly available in the 1980s through the use of recombinant deoxyribonucleic acid (DNA) technology. In this technique the gene specifying human insulin is spliced into the chromosome of a bacterium, and the billions of progeny bacteria then produce insulin as though it were one of their own bacterial proteins, thus serving as minifactories for the hormone. The bacterium used to produce insulin is Escherichia coli. Another DNA technique for producing insulin uses yeast instead of E. coli. Up to the early 1980s, insulin was extracted from cattle and pigs. This “foreign” insulin is still used, but has some unwanted side effects not seen or rarely seen with human insulin, therefore making human insulin the treatment of choice. One of the most important characteristics of insulin produced by genetic engineering, other than its being identical to human pancreatic insulin, is its limitless availability. See also: Genetic engineering; Insulin; Pancreas
Diabetes mellitus type 2
diabetes mellitus type 2
Type II is the more common form of diabetes mellitus, accounting for 8 out of every 10 cases. It usually appears after the age of 30, although an uncommon variant called type II diabetes of the young occasionally occurs in obese children and teenagers. The initial symptoms of type II diabetes are much less noticeable than those of type I, and the characteristic triad of polyuria, polydipsia, and polyphagia may even be entirely absent. For this reason, type II diabetes can exist undetected for dangerously long periods. Victims are not prone to the ketoacidosis and coma that threaten type I patients, and their disease can usually be managed without insulin injections. Thus two other names for type II diabetes are nonketosis-prone diabetes and noninsulin-dependent diabetes.
Whereas type I diabetes is a disease of insulin shortage, victims of type II diabetes usually have insulin in their bloodstream. In fact, insulin levels in type II diabetics are sometimes even higher than those in nondiabetic individuals. However, since the cells of a type II patient do not respond to insulin by taking in and utilizing blood glucose as normal cells would, the type II diabetic may have hyperglycemia in spite of high insulin levels. The probable reason for this defect is that the cells have specific receptor molecules on their surface membranes whose job is to recognize insulin and trigger the biochemical steps leading to glucose uptake and utilization. Interestingly, the number of insulin receptors on cells can be changed by gaining or losing body weight; the more body fat a person carries, the fewer insulin receptors there will be on the cells. This may explain why type II diabetes is mainly a disease of the obese, and why weight reduction is such effective therapy. High glucose levels also decrease the number of insulin receptors; normalizing glucose levels is thus of utmost importance.
The most important treatment for most cases of type II diabetes consists of exercise and weight reduction, which will return glucose metabolism to normal in 9 out of 10 cases. Because the cells of type II diabetics lack responsiveness to their own insulin, insulin injection therapy is used for some of these cases.
Approximately 10% of all type II patients must use insulin. This percentage appears to more than double in Black, Latino, Native American, or other minority patients living in the United States. In addition, a family of drugs known as oral hypoglycemic agents is often used in treating the disease. These drugs, including tolbutamide, chlorpropamide, acetohexamide, and tolazamide, lower blood glucose by stimulating the pancreatic cells to release insulin, and by augmenting insulin's effect on the cells of the body. All of these drugs are known as first-generation sulfonylureas. However, there are other drugs with the same basic molecule but with chemical changes in their structure; these are called second-generation sulfonylureas. This group of drugs is safe if properly used and is effective in many cases if used in conjunction with proper diet and exercise programs.
Amylin
Amylin is a 37-amino-acid peptide hormone that occurs naturally in humans, and has been shown to be in excess in individuals with non-insulin-dependent diabetes mellitus. Amylin has been shown to be deposited in the islets of Langerhans, and may decrease insulin release and insulin production in the pancreas, thus causing a deterioration in glucose control in non-insulin-dependent diabetes.
In insulin-dependent diabetes, amylin appears to slowly decrease with the progression of the disease, and when none is found, individuals may be more prone to have hypoglycemia unawareness (low blood glucose levels without symptoms).
Complications
Both type I and type II diabetes tend to produce a number of debilitating and life-threatening complications despite the use of insulin or oral hypoglycemic agents. It is primarily these complications, not the risk of ketoacidosis, that account for the heavy burden this disease inflicts on society, and make diabetes the third leading cause of death in the United States.
Much evidence indicates that most of the complications of diabetes are caused by the elevated blood glucose levels common in this disease. Even diabetics who take regular insulin injections exhibit wide fluctuations in their blood glucose levels, in marked contrast to the tightly controlled blood glucose levels observed in nondiabetics. According to the prevalent hypothesis, the more diabetics succeed in controlling their blood glucose to near-normal levels, the less risk there will be of developing any complications of the disease.
Thus, careful attention to diet, exercise, regular medication, and monitoring of blood glucose is vitally important for any diabetic.
The most common complications of diabetes are the following.
Eye damage
Diabetes is the leading cause of nontraumatic blindness in young adults. The blood vessels of the diabetic eye
are prone to microaneurysms (small outpouching of the vessel wall), excessive vascular permeability
(leakage from the vessel), growth of newer, more fragile vessels, and ultimately hemorrhage (bleeding).
These events can lead to scarring, fibrosis, and subsequent loss of vision.
Kidney damage
In long-standing diabetes, the smallest blood vessels of nephrons (the functional filtration units of the
kidney) frequently suffer the same type of damage as the blood vessels of the retina; this condition is called
diabetic nephropathy. Severe diabetic nephropathy commonly leads to kidney failure, and such patients
require dialysis in order to survive. The prognosis for individuals with diabetes on dialysis is poor, with only
30% surviving beyond 5 years.
Premature atherosclerosis
Atherosclerosis (often called arteriosclerosis or hardening of the arteries) is a condition in which arteries
become progressively occluded by accumulations of cholesterol-containing plaque. Although atherosclerosis is
common in older nondiabetics, diabetics tend to develop it earlier and in a more severe form. The most
common consequence of atherosclerosis is coronary artery disease and stroke, which result when the blood
supply to the heart or the brain is obstructed by a plaque within an artery. Coronary artery disease is the
leading cause of death in long-term diabetics, accounting for 75% of fatalities. Also, because of
atherosclerosis and restricted blood flow, diabetics are often subject to gangrene, especially of the
extremities. See also: Arteriosclerosis
Nervous system abnormalities
Patients with diabetes may experience a variety of nervous system disturbances, collectively referred to as
diabetic neuropathy. Symptoms may include muscle weakness, pain in the extremities, local paralysis,
urinary incontinence, sexual impotence, and sensations of cold, heat, or tingling in various parts of the body.
There may also be episodes of diarrhea, frequently nocturnal, which is a characteristic of the “diabetic
diarrhea” problems involving the upper intestinal tract. Nervous system involvement of the esophagus and
stomach may cause nausea and even vomiting.
Causes
Three factors that are believed to be important in the causation of this disease are heredity, viral infections,
and immunological damage to the pancreas.
Heredity
Although diabetes is popularly considered a genetic disease, it is not inherited in the sense that one can
inherit curly hair. Heredity does operate in determining one's risk of diabetes, but only as a predisposing
factor, not as an absolute determinant. The two types of diabetes mellitus have entirely different patterns of
inheritance, and the presence of one type in a family does not influence one's risk of developing the other.
Genetic factors play a much more important role in type II diabetes than in type I diabetes. For example, the
identical twin of a person who develops type II diabetes after age 40 is almost 100% certain to develop the
disease, but someone whose identical twin has type I diabetes runs only a 52% risk of becoming a diabetic.
Parents with type I diabetes face only a 2% risk of having a child with the disease, whereas the risk to the
offspring of a type II diabetic is about 10%. Genetic predisposition is apparently stronger in the case of type
II diabetes of the young, with a 50% chance that the child of such a diabetic will also develop the disease.
The environment obviously plays a significant role in type II diabetes. See also: Human genetics
Virus infections
Virus infection is strongly implicated as one causative factor in the beta-cell destruction that characterizes
type I diabetes, but it is not involved in type II diabetes. Some of the viruses that have been implicated are
the agents of mumps and rubella (German measles), whose action seems to be delayed for months or years,
and coxsackievirus B, which is more likely to precipitate diabetes shortly after the person recovers from the
influenzalike infection. Apparently, several factors operate to determine whether or not diabetes will develop
in a person infected with one of these extremely common viruses. They include the organ affinity of the
particular virus strain, the person's susceptibility to viral invasion of the pancreatic tissue, and the individual's
capacity to regenerate islet tissue that has been damaged by a viral infection. See also: Animal virus
Immunological damage to pancreas
Autoimmune reactions, wherein the body's immune defense system attacks its own pancreatic tissue as
though it were a foreign substance, are also suggested as a cause for the beta-cell destruction of type I
diabetes. An autoimmune response may be conducted by T lymphocytes or by soluble antibodies in the blood
or by both. These reactions may arise spontaneously or may be secondary to a viral infection of the pancreas
that leaves the islet tissue modified in some way that marks it for attack. See also: Autoimmunity
Diet
Dietary management has been part of diabetic therapy since preinsulin days, when starvation diets were
used to prolong the life of type I diabetics. More recently, weight reduction for victims of type II diabetes and
complex carbohydrate liberalization for those of both types of diabetes mellitus have been the cornerstone of
therapy.
For obese type II diabetics, weight reduction is certainly appropriate, since it tends to increase the number of insulin receptors on the cells of the body, usually making it possible to normalize blood glucose without
resorting to the use of insulin injections or oral drugs.
Some other dietary measures besides reducing caloric intake are now believed beneficial for type II diabetics.
The ingestion of foods high in fiber content, for example, has been shown to reduce hyperglycemia in type II
diabetics.
For type I diabetics, the traditional diet is high in protein and quite restricted in carbohydrates, with only
about 45% of the total daily caloric intake being carbohydrate-derived. Since most type I diabetics are thin,
weight reduction is not part of their program. Presently, the recommended carbohydrate intake has been
liberalized to 55–60% of the diet, plus 15–20% protein and 20–30% fat. There has been a trend toward
relaxing the carbohydrate restriction for type I diabetics as evidence accumulates that diets containing even
as much as 80% carbohydrates can be compatible with excellent control of diabetes, as long as the
carbohydrates are complex (that is, whole grains, legumes, potatoes, bread) rather than refined (that is,
sugars, candy, soft drinks, desserts, and so on). Artificially sweetened food can be very beneficial for weight
control; however, it is not a necessary component of treatment.
Prospects
The ideal solution is to be able to mimic insulin secretion, with intensive insulin therapy used with either
multiple insulin injections or insulin infusion pump therapy. The insulin pump continuously delivers a small
amount of insulin, and the individual can increase the amount before meals based on his or her glucose level.
Still, this setup is not ideal: in a nondiabetic, insulin is delivered directly into the portal blood system, while
therapy delivers insulin under the skin, where it can be absorbed into the bloodstream. Hooking a glucosemonitoring
device to the insulin pump would allow the system to close, permitting the individual to have an
artificial pancreas implanted (several models are available).
Healthy pancreatic tissue can be transplanted from a donor into a type I diabetic, but there are many
problems related to this method, such as the typing of the pancreatic tissue from the donor, the possibility of
rejection, and the possibility of infections.
diabetes mellitus
Diabetes Insipidus
Diabetes insipidus is caused by a deficiency of, or resistance to the action of, vasopressin, the antidiuretic
hormone produced by the posterior lobe of the pituitary gland. If the pituitary fails to produce vasopressin,
the condition is called central diabetes insipidus. If the kidneys do not respond to the vasopressin and fail to
concentrate urine, the condition is labeled nephrogenic diabetes insipidus. Symptoms include increased thirst
and frequent urination. Permanent damage to the kidneys can result if the condition is not treated.
A low level of vasopressin can be corrected with desmopressin acetate, a synthetic analog of 8-argininevasopressin,
which can be administered in the form of a nasal spray. Desmopressin acetate is ineffective
in the treatment of nephrogenic diabetes insipidus. See also: Neurohypophysis hormone
diabetes mellitus - diabetes mellitus type 2 - diabetes mellitus type 1









{kind=link}