The basics of bone marrow transplants
A bone marrow transplant (BMT) is a fairly new treatment for diseases that until recently could not be cured. Since it was first used with good results in 1968, this treatment has been used for patients with immune system diseases and blood diseases such as leukaemia, lymphoma and multiple myeloma.

In Australia each year, around 1,000 children and adults have a BMT. More than 300 people have a BMT each year in New South Wales.
What is bone marrow?
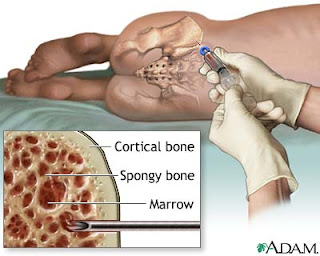
Bone marrow is the soft, spongy part in the centre of your bones where blood cells are produced. The bone marrow makes stem cells, which are early-stage cells that produce other cells. Each tissue in the body contains stem cells that renew and replace that tissue when needed due to damage or wear and tear. Stem cells generate all blood cells in the human body, including red cells, white cells and platelets.
Types of BMT
Allogeneic transplant
This type of transplant uses stem cells donated by another person (a donor) and is the focus of this book. It is called a syngeneic transplant if the donor is an identical twin.
The two types of allogeneic transplants are:
• Myeloablative or full allo: the aim is to destroy the patient’s marrow and kill the cancer cells.
• Non-myeloablative (“mini” allo): the aim is to suppress the patient’s marrow and allow the donor cells to grow and attack the cancer cells. This is the graft-versus-tumour effect.
There are two ways to collect or harvest the donor’s stem cells:
�� A peripheral blood stem cell harvest: this is used for most adult transplants and collects stem cells from the donor’s circulating blood.
�� A bone marrow harvest: this collects stem cells from the donor’s bone marrow, usually from the hip bones.
The donor’s stem cells must match the genetic make-up of your own cells as closely as possible. Blood tests, called tissue typing, are done to work out if the donor’s cells match.
The most suitable donor is usually a brother or sister whose bone marrow is a close match. There is a 25-35% chance that a patient will have a family member whose stem cells match. But if no matching relative can be found, an unrelated donor may be found in the Australasian/International Bone Marrow Donor Registry. A mismatched or autologous BMT may also be considered.
The basics of bone marrow transplants
The basics of bone marrow transplants
The basics of bone marrow transplants
Autologous transplant
An autologous transplant uses your own stem cells. This type of transplant can be done if the disease is in remission or if the illness does not involve the bone marrow (eg, Hodgkin’s disease, non-Hodgkin’s lymphoma).
For an autologous BMT, stem cells are taken from the patient’s blood before the transplant, stored and then given back after high-dose chemotherapy or radiotherapy.
This book does not describe autologous BMT in detail. For more information about autologous transplants, see the BMT Network NSW publication, Autologous Bone Marrow Transplant: A Patient’s Guide.
Preparing for a BMT
The BMT team
An expert team of doctors, nurses and other support staff will care for you. The team can quickly identify and treat any problems or side effects. A good BMT program will also give patients and their families emotional and psychological support before, during and after the transplant.
For a BMT to work well, you must be healthy enough to cope with the procedure. When deciding if you should have a BMT, your doctor will consider your age, general physical condition and the type and stage of your disease.
The work up
Before a BMT, a number of tests are carried out to ensure you are healthy enough for the treatment. You will also have tests of heart, lung and kidney function before and after the BMT so your doctor can check whether these organs are still working as well after the transplant. The pre-BMT tests (also called the work up) are usually done before you are in hospital, but may be done after you are admitted.
You will need to have a dental check-up and all necessary work done before the BMT. If you or your dentist is unsure, please check with your BMT team before any work is started.
The basics of bone marrow transplants
Making informed decisions
Long-term implications
It is important to think about some of the possible long-term effects, such as infertility, and discuss them with your transplant doctor before starting a BMT. See page ?? for more information.
Gathering information
When you are considering a BMT, you will be given a lot of information about the process. Some people do in-depth research and think through every detail, while others just want enough information for the next day or stage. Some people only want to know enough to be informed, and choose not to read or listen to anything negative so they can stay motivated and focused.
A BMT is a serious and complicated procedure so it is vital you are informed and that you clearly understand what the BMT means for you. This requires good communication with your BMT doctor and the rest of the team.
At your first visits to the doctor, you will receive a lot of information about the proposed BMT, its side effects and possible complications. To help you absorb this information, it can help to take notes during the consultation or tape-record the discussion. Many people like to have a relative or friend go with them, to take part in the discussion, take notes or just listen.
If you don’t understand what you’ve been told, don’t be afraid to ask questions or to ask for the information to be repeated as often as you need. Questions are a good sign that you are working in partnership with your medical team. It is very important to be involved in your care and to express your concerns before, during and after a BMT. Your role is crucial, particularly in telling the team about how you are feeling and any symptoms you are having.
In the days before the BMT, you will need to sign a number of consent forms for the treatment or clinical trial.
Finally, remember that not everyone will want to go ahead with a BMT. After thinking about all the possible risks and benefits, some people decide it is not for them. In this case, you need to tell your doctors, and talk to them about other treatments. Your doctor will still give you the best other treatment options available.
How is a BMT done?
Collecting bone marrow stem cells
The stem cells are collected from the donor’s blood or bone marrow. If the donor is related to you, the stem cells will usually be collected from the blood. Cells from unrelated donors are harvested from the either the peripheral blood or the bone marrow, under general anaesthetic, depending on what your doctor believes is best for you and/or donor preference.
The central line
If you don’t already have one, a central venous catheter will be inserted under the skin of your chest into a vein. It is also called a central line or Hickman catheter depending on the type of line.
A central line is a long, hollow tube that usually has two or three passages (called lumens) to allow for a number of uses. It is made of silicone or hard plastic. Your central line will stay in place during the BMT and may be used to collect blood samples and to give you all the medications and fluids you need.
Your central line will usually be inserted into a large vein that runs beneath your collar bone with the tip sitting near to the entry into your heart. The rest of the central line remains outside your body for easy access. A clamp keeps the tube closed when it is not being used. The central line may be put in when you are in the operating theatre, in the x-ray department or on the ward.
Add diagram showing central line in place
Conditioning treatment
You will have several days of chemotherapy and/or radiotherapy, which destroy bone marrow and cancerous cells and make room for the healthy stem cells. This is called the conditioning or preparative regimen.
You may also hear the phrase ‘countdown to transplant’, because this treatment is expressed in your medical notes in terms of the number of days until the transplant. For example, day -5 (minus 5) means that you are five days away from the transplant day, which is called day 0. The type and number of days of chemotherapy and/or radiotherapy vary according to the disease being treated and the protocol or preferred treatment plan of the hospital where the BMT is being done.
For a myeloablative BMT, the dose of chemotherapy and/or radiotherapy given to patients during conditioning is much stronger than doses given to patients with the same disease who are not having a BMT. You may become weak, irritable and nauseous. Anti-nausea medications will help during this period. Don’t be alarmed if your blood results go down at this time, as this is what the chemotherapy or radiotherapy is supposed to do – that is, empty your bone marrow before your transplant.
The transplant
The transplant will take place a day or two after the chemotherapy and/or radiotherapy. The transplant is not a surgical procedure. It takes place in your hospital room, not an operating room.
You may be given medication before the transplant to prevent a reaction to the transplanted cells. This is more likely to occur when the match between the donor marrow and the patient is not exact or the blood groups are different.
The healthy bone marrow stem cells are infused through your central line, in much the same way that any blood product is given. Many patients describe the actual transplant as an anticlimax, as it all over so quickly – usually between 30 minutes and an hour.
You will be checked frequently for signs of fever, chills, hives and chest pains while the bone marrow is being infused. When the transplant is completed, the days and weeks of waiting begin.
The bone marrow begins to grow (engraftment)
Engraftment means new cell growth. It takes place after your bone marrow transplant when there is a sustained rise in new blood cell production. As a general guide, engraftment is said to have happened once the white blood cell count rises above 0.5 x 10 9 /L and the platelet count to above 20 x 103 /L without transfusion.
The 2-4 weeks after the transplant are the most critical. The high-dose chemotherapy and/or radiotherapy given to you during conditioning destroyed your bone marrow, crippling your immune or defence system, leaving your body with no natural defences against infection.
As you wait for the transplanted bone marrow to migrate to the cavities of the large bones, engraft and begin producing normal blood cells, you will be very susceptible to infection and excessive bleeding. You will be given multiple antibiotics and blood transfusions to help prevent and fight infection. You will also have transfusions of platelets to prevent bleeding and additional medications to prevent and control graft-versus-host disease (GVHD), which happens when the white blood cells from the donor marrow attack the cells of the patient’s body. (For detailed information of GVHD, see page?)
While many infections start from within the body, your BMT team will take a number of precautions to minimise your exposure to viruses and bacteria in your environment. These will vary from centre to centre. Visitors and hospital personnel will wash their hands with antiseptic soap and may wear protective gowns, gloves and/or masks while in your room.
Any visitors or relatives will be asked not to visit if they are unwell eg, if they have a sore throat, runny nose, a cold /flu or upset stomach. Fresh fruits, vegetables, plants and cut flowers, which often carry fungi and bacteria that pose a risk of infection, may not be allowed in your room.
When leaving the room, you may wear a mask, gown and gloves as a barrier against bacteria and virus, and also to remind others that you are susceptible to infection.
Blood samples will be taken daily to monitor engraftment and organ function. When the transplanted bone marrow engrafts and begins producing normal blood cells, you will gradually be taken off the antibiotics, and blood and platelet transfusions will generally no longer be required.
Once the bone marrow is producing a sufficient number of healthy red blood cells, white blood cells and platelets, you will be discharged from the hospital, provided no other complications have developed. BMT patients typically spend 4-8 weeks in hospital.
How you may feel physically during the transplant
A BMT is a physically, emotionally and psychologically taxing procedure for you and your family. Seek as much help as you need to cope – toughing it out on your own is not usually the best way to cope with the transplant experience.
At times, you may feel very sick and weak during the transplant. Walking, sitting up in bed for long periods of time, reading books, talking on the phone, visiting with friends or even watching TV may require more energy than you have.
Complications can develop after a bone marrow transplant such as infection, bleeding, GVHD or liver disease, which can create additional discomfort (see page?). Pain is usually controlled with medication, which may include the use of intravenous morphine or other narcotic drugs. In addition, mouth and throat sores can develop that make eating and swallowing uncomfortable and difficult. Temporary mental confusion sometimes occurs and can be frightening for the patient who may not realise it is only temporary. The medical and nursing staff will help you and your carers deal with these problems.
Dealing with emotional and psychological concerns
Being diagnosed with a life-threatening illness can be a traumatic experience. It is common to feel overwhelmed by the amount of information you receive and the need for urgent treatment. Each person feels differently and responds differently. People will find some aspects of the treatment process more stressful than others.
It is important you know that BMT is a team effort and that you are the central and most important person in this team. Understanding your treatment plan and clear communication are essential elements in maintaining your emotional and psychological well-being. People often say it is the unexpected symptom, complication and treatment that upsets or frightens them the most. A BMT already involves a degree of uncertainty. Poor communication can add unnecessary stress to this situation. Don’t hesitate to clarify any aspect of the process.
People will vary in the amount of information they want about the transplant. Some will want to speak to others who have been through a bone marrow transplant. Some will want to be well researched on all aspects of the transplant process. Others will only need to have minimal facts about their proposed treatment. Whichever category you fall into, it will be important for you to have all the information you need about your treatment before the transplant.
You may find that you feel isolated with little control over your day-to-day activity because of the precautions taken to guard against infection while your immune system is not working properly. You will be in a single room and the number of visitors you can have at one time is restricted.
Make your room your own space with your personal effects. Try to stay as independent as you can and talk to your nurses about how you can participate in your care. Lack of privacy is another common issue for people having a BMT – talk to your nurse about allocating times when you will be as undisturbed as possible.
Waiting for the transplanted stem cells to engraft, for blood counts to return to safe levels or for side effects to disappear can be very frustrating and lead to increased stress. Try to remain positive and be realistic in your goals. BMT is an individual process that cannot be predicted all of the time.
You may find that personal relationships with family and friends come under pressure during BMT. This is not uncommon. Relationships within families will change, and it is important to recognise what these changes will be. Talk to the BMT social worker if you need help.
Each family member or close friend will cope with your BMT in their own way and this may, at times, lead to misunderstandings or conflict. Just because a family member or friend is not visiting does not mean they don’t care – they may just be taking some time out as their way of coping.
Psychological discomfort, like physical discomfort, is a normal symptom of the BMT experience. Social workers and psychologists/psychiatrists are also part of your BMT team, so call on them when you need help. There is no right or wrong way to manage all the challenges and stresses that BMT throws at you. There is only the method that works for you.
Going home
Recovering from a BMT continues for some months after you leave hospital. For the first few weeks you may be too weak to do much more than sleep, sit up and walk a bit around the house. You will need to visit the hospital or clinic regularly so your BMT team can monitor your progress and administer any medications and/or blood products needed.
It will take at least six months before you will be ready to return to work or your normal daily activities. You’ll need lots of patience and determination to cope during this period. Some people find that reaching their ‘new normal’ takes longer than others.
Your new marrow is still in its infancy and is not yet able to protect you from some bacteria and viruses encountered in everyday life. The medications you will need to control GVHD only add to this. So it is important to protect yourself from potential sources of infection. Enjoy the outdoors, dine alfresco, keep sick friends and relatives away, see movies and do the shopping at quiet times. You can get back to a normal life; you just have to take a little extra care.
Life after BMT
Life after transplant can be both exhilarating and stressful. On the one hand, it is exciting to be alive after being so close to death, and many people find their quality of life has improved after transplant.
But there is always the worry that a relapse will occur. Also, innocent statements or events can sometimes conjure up unpleasant memories of the transplant experience long after recovery. It can take a long time to come to grips with these difficulties. Tell your BMT team about any difficulties you experience.
Shaded box
Frequently asked questions
What is a bone marrow transplant (BMT)?
A BMT is a standard treatment option for some people who have life-threatening blood or immune system diseases. It is the process of replacing unhealthy bone marrow cells (stem cells) with healthy bone marrow cells. The healthy bone marrow cells are re-infused intravenously after very strong chemotherapy and/or radiotherapy, which kills your unhealthy bone marrow cells. The re-infusion of healthy bone marrow cells essentially rescues you from your chemotherapy and/or radiation by enabling your bone marrow to start producing new red and white blood cells and platelets.
What is the difference between a BMT and a peripheral blood stem cell transplant?
Both transplants aim to do the same thing – replace bone marrow stem cells in a person who has had their bone marrow destroyed by large doses of chemotherapy and or radiotherapy.
Bone marrow is the spongy substance found in the hollow of bones of the hips, legs and arms. It contains stem cells (also called CD34s), which produce all circulating blood cells: red blood cells, white blood cells and platelets.
When the stem cells are collected from circulating blood, the transplant is called a peripheral blood stem cell transplant. A transplant with stem cells collected from the marrow, usually from the hip bone area, is called a bone marrow transplant.
Are there different types of BMT?
Yes, there are two different types of BMT. This book focuses on allogeneic bone marrow transplant, which involves finding a donor whose tissue type closely matches yours. The donor can be related or unrelated. Related donors are usually a brother or sister. If no matching relative is found, your transplant doctor will ask the Australian Bone Marrow Donor registry to start a search (see Finding a donor, page ?). An autologous BMT uses your own blood stem cells, but this type of transplant is not discussed in this book.
If I have a common blood group, will I have a common tissue type?
No, not necessarily. There is no link between your blood type and your tissue type. Tissue type is determined by different sets of genetic proteins called human leukocyte-associated antigens (HLA), which are found on the surface of most cells. A person’s tissue type is identified by a blood test called tissue typing. Therefore, your donor can still be a bone marrow match for you but have a different blood group.
Will I need an operation to have a BMT?
No, the stem cells will simply be re-infused through your central line in the same way you receive transfusions such as platelets or red blood cells (packed cells).
What is engraftment and when will it happen?
Engraftment means new cell growth, and takes place after your bone marrow transplant when there is a sustained rise in new blood cell production. This generally occurs within 2-4 weeks after your transplant. The first obvious sign may be a rise in your white blood cell count above 0.5. This tells us that your new bone marrow cells are starting to produce new blood cells. Until this time, you are at high risk of infection and need to avoid possible sources of infection.
What are the possible side effects of a BMT?
The two main risks from the transplant process are an increase risk of infection and bleeding due to high doses of chemotherapy and/or radiation. Short-term effects may include nausea, vomiting, fatigue, mouth ulcers, weight loss, hair loss and skin reactions. Long-term effects include infertility, cataracts and possible complications in the liver, kidneys, lungs, joints and/or heart.
Allogeneic transplants carry the risk of GVHD. This occurs when the white blood cells from the donor marrow (the graft) identify the cells of the patient’s body (the host) as foreign and attack it. This can be mild in the form of skin rashes on the hands and feet, to very severe affecting liver, gut and/or lung function. (For detailed information about possible BMT complications, see page??)
What are my chances of having a successful BMT?
This is very difficult to answer as so many individual issues come into play. The outcome of your transplant is highly influenced by your original disease, the stage of your disease and your general condition at the time of the transplant. There are many other variables, including how you have responded to treatment and the closeness of the match of your donor. The best person to discuss your possible transplant outcome is your transplant doctor. He/she can discuss your individual factors that may influence your chances of success.
The basics of bone marrow transplants
The basics of bone marrow transplants









 is a fairly new treatment for diseases that until recently could not be...){kind=link}